Topic: COMMUNITY INTEREST

Hamilton Leadership Ignores Lead Laws
By Tammy Duffy
The man-made drinking water crisis in Flint has made international headlines. For more than a year, state officials -- from Gov. Snyder to his appointed Flint emergency managers to the Michigan Department of Environmental Quality -- exposed an entire city to the risk of lead poisoning in their drinking water. It's a public health catastrophe with long-lasting consequences for the children under the age of six in Flint who will suffer neurological damage for the rest of their lives.
A Hamilton resident, age 4, died in his sleep Sept. 25 from EVD68. In 2014, the United States experienced a nationwide outbreak of EVD68 associated with severe respiratory illness. For months prior to the death of a Hamilton resident, there was a nationwide epidemic occurring. The CDC was contacting the nation and health workers on how to help elevate this epidemic in towns. Several health departments and mayors in towns in Mercer county, not including Hamilton, were proactive in educating their schools, residents know what to do as it pertained to hand washing and cleanliness. The township of Hamilton was silent on this issue. There were zero proactive measures made during the EVD68 outbreak. It was not until after the death of a 4 year old resident that the local health department and mayor made any type of announcement or educated the community.
During several of the press conferences, after the death of a resident, the mayor of Hamilton Township, stated, "Does anyone even know what EVD68 is? This was a startling statement for residents. How can the leader of a town, when a nationwide epidemic is occurring not know about it? This same leader was oblivious to the fact that there was a heroin epidemic in her own town and named her town, "the Big H" at another press conference. "The Big H" is the street name for heroin. What does this leader know about the lead crisis in America? There is zero information on the township website to educate residents on what to do for their children as it pertains to lead in the water. Upon calling the HAMSTAT headquarters and the Department of Health in Hamilton we learned that there are nothing as well. The people we spoke to knew of no programs, mandatory testing or could speak to the results demonstrated in the NJ State Department of Health report. Is Hamilton the next Flint? Why are the children not being tested? Where is the plan to protect the residents?
N.J.A.C. 8:51A requires the protection of children less than six years of age from the toxic effects of lead exposure by requiring lead screening pursuant to N.J.S.A. 26:2-137.2 et seq. (P.L. 1995, c 328. An EBLL: Elevated Blood Lead Level is 10 µg/dL or greater.
The number of children tested for lead in NJ as 220,787, which represents an increase of 2.9% over the 214,478 children tested during SFY 2011. The SFY 2012 number of children tested also includes 103,380 children, or 48%, who are between six and 29 months of age, the ages at which all children must be tested under State law.
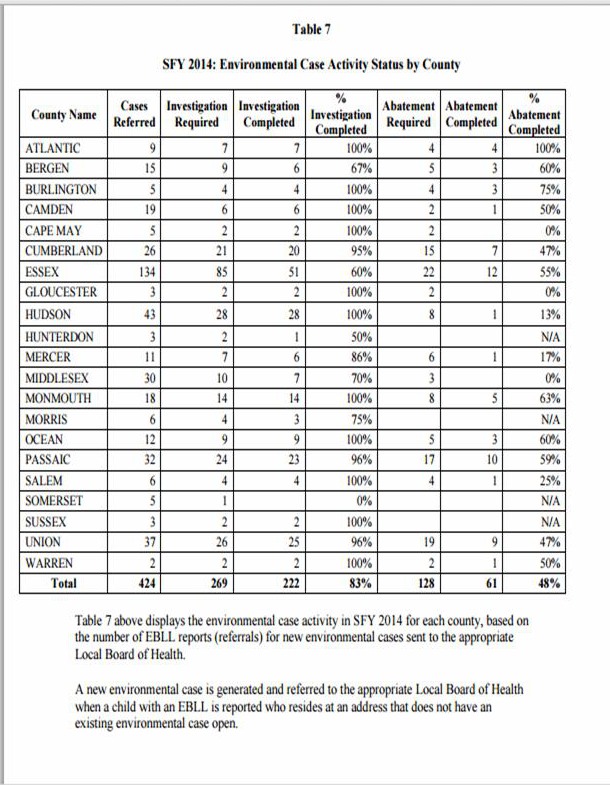
While 213,020 (99.5%) children tested during SFY 2012 had blood lead levels below the Centers for Disease Control and Prevention (CDC) threshold of 10 μg/dL, there were 1,155 (0.52%) children with a test result above this threshold, including 236 children, who had at least one test result of 20 μg/dL or greater. In 2014, only 83% of the investigations of Pb levels above 20 μg/dL in NJ were completed. However, only 48% of the abatements were completed according to a Department of Health report from 2014. The reports states that this lack of follow up are occurring due to the following issues:
- difficulty in identifying and communicating with absentee property owners
- lengthy enforcement actions and court proceedings against recalcitrant property owners;
- delays in contracting with and scheduling work to be performed by State-certified lead abatement contractors; and, inability of property owners to obtain financial assistance to pay for the cost of the required abatement
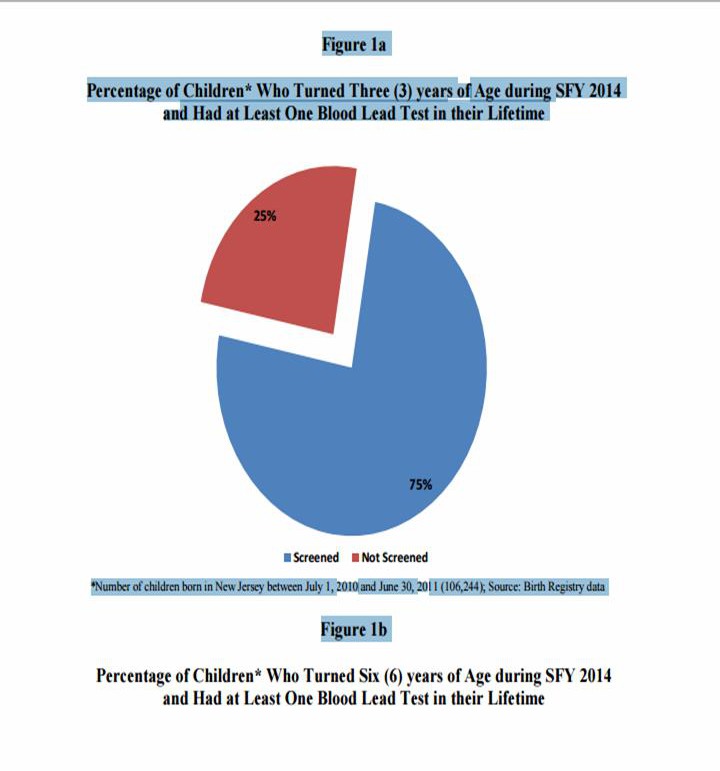
In New Jersey, all children are to be tested at both one and two years of age. At a minimum all children should have at least one blood lead test before their sixth birthday. Approximately 78% of children in New Jersey have had at least one blood lead test prior to reaching three years of age. In Hamilton the numbers are significantly lower. The numbers are as low as 14% of children being tested. There was a new gun range built in a residential neighborhood in Hamilton, costing more than $500,000 according to sources. There are two other ranges within 3 miles of the town that the township police could use. Why was this money spent on a range vs. the children to get them tested?
Lead is a heavy metal that has been widely used in industrial processes and consumer products. When absorbed into the human body, lead affects the blood, kidneys and nervous system. Lead’s effects on the nervous system are particularly serious and can cause learning disabilities, hyperactivity, decreased hearing, mental retardation and possible death. Lead is particularly hazardous to children between six months and six years of age because their neurological system and organs are still developing. Children who have suffered from the adverse effects of lead exposure for an extended period of time are frequently in need of special health and educational services in order to assist them to develop to their potential as productive members of society. The primary method for lead to enter the body is the ingestion of lead containing substances.
Lead was removed from gasoline in the United States in the early 1980’s. This action is credited with reducing the level of lead in the air, and thereby the amount of lead inhaled by children. However, significant amounts of lead remain in the environment where it poses a threat to children. Some common lead containing substances that are ingested or inhaled by children include:
· lead-based paint
· dust and soil;
· tap water;
· food stored in lead soldered cans or improperly glazed pottery
· traditional folk remedies and cosmetics containing lead.
All children in New Jersey are at risk because lead-based paint and other lead-containing substances are present throughout the environment. Some children, however, are at particularly high risk due to exposure to high dose sources of lead in their immediate environment.
These potential high dose sources include: leaded paint that is peeling, chipping or otherwise in a deteriorated condition; lead-contaminated dust created during removal or disturbance of leaded paint in the process of home renovation; and lead-contaminated dust brought into the home by adults who work in an occupation that involves lead or materials containing lead, or who engage in a hobby where lead is used. Recently, there has been much attention focused by the media on the increasing number of foreign imports coming into the United States being tainted with dangerous levels of lead.
This has been alarming especially when these imports consist of toys and other products used primarily by children. However, in New Jersey, today, the primary lead hazard to children comes from leadbased paint. In recognition of the danger that lead-based paint presents to children, such paint was regulated for residential use in New Jersey in 1971, and banned nationwide in 1978. There are numerous dollar stores in the township of Hamilton that carry many of these lead contained toys that the children are playing with.
This ban has effectively reduced the risk of lead exposure for children who live in houses built after 1978, but any house built before 1978 may still contain leaded paint. The highest risk for children is found in houses built before 1950, when paints contained a very high percentage of lead. There are nearly one million housing units in New Jersey, 30% of the housing in the state, which were built before 1950. Every county in the State has more than 9,000 housing units built before 1950 and more than 2.5 million housing units built prior to 1980


New Jersey Takes Childhood Lead Poisoning Seriously By Acting Health Commissioner Cathleen D. Bennett Every day in New Jersey, in local health departments, community health centers, doctors’ offices, WIC clinics and in home visits with at-risk populations, health professionals test children for elevated lead levels and educate families about preventing lead poisoning, which can cause behavior and learning problems, lower IQ, hyperactivity, slowed growth, hearing problems, anemia and kidney damage. New Jersey is one of 17 states that require universal lead screening of all children at ages 1 and 2.
Other states target screening only to children at increased risk for lead exposure. New Jersey’s approach is far more protective. More than 205,600 children were screened for lead last year. And the number of children with elevated blood lead levels has dramatically declined over the past 20 years.
There were 27,295 cases in 2000 compared to 3,426 so far this year. That is a public health success story. More than 100 WIC clinics in New Jersey ask every mother and caregiver if their child has been tested for lead. If they have not, they are referred to a clinic or to their physician for testing. If their child’s test shows elevated levels, they are counseled on the importance of nutritious foods rich in Iron, Vitamin C and Calcium and warned about potential sources of lead exposure such as chipping paint and imported products. Each year, the Department of Health provides $11 million to the Department of Children and Families to support its evidence-based home visitation programs, which bring nurses, community health workers and, in some cases, trained parents into the homes of at-risk families to provide information and referrals on child health and safety issues including strategies to reduce exposures to lead. New Jersey’s poison control center, the New Jersey Poison Information and Education System (NJPIES), has used state funding for years to educate the public on lead poisoning and to counsel callers to its 24/7 hotline (1-800-222-1222). It has also issued numerous warnings about non-traditional sources of lead including imported candies, jewelry, cosmetics, spices, pottery and home remedies. The Department also funds continuing medical education so that health care providers understand how to identify lead poisoning. Yet, there is zero information in Hamilton to educate the residents.
After Superstorm Sandy devastated New Jersey—heightening the risk of lead exposure due to extensive debris from thousands of destroyed homes and businesses--the Department of Health asked the federal government for and received $5.4 million for a Lead Poisoning Prevention Initiative.
According to a report by the N.J. Department of Health from 2014, the township of Hamilton demonstrated they had 1,814 children who were in the age bracket of 6 to 26 months of age. Only 22% of these children were tested for lead. These results demonstrate one of the lowest in the state out of the large municipalities evaluated.
- 392 children in this age bracket were found to have lead levels below 5 BLL (µg/dL)
- 9 children in this age bracket were found to have lead levels between 5-9 BLL (µg/dL)
- 1 child in this age bracket were found to have lead levels above10 BLL (µg/dL)
- Only 22% of the children were tested
N.J.A.C. 8:51A requires the protection of children less than six years of age from the toxic effects of lead exposure by requiring lead screening pursuant to N.J.S.A. 26:2-137.2 et seq. (P.L. 1995, c 328. So why is the Township of Hamilton ignoring this law? Why are only 22% of the children being evaluated in Hamilton township, Mercer County?
According to a report by the N.J. Department of Health from 2014, the township of Hamilton demonstrated they had 5,480 children who were in the age bracket of less than 6 years of age. Only 14.9% of these children were tested for lead in Hamilton township, Mercer County. These results demonstrate one of the lowest in the state out of the large municipalities evaluated.
- 749 children in this age bracket were found to have lead levels below 5 BLL (µg/dL)
- 18 children in this age bracket were found to have lead levels between 5-9 BLL (µg/dL)
- 1 child in this age bracket were found to have lead levels above10 BLL (µg/dL)
- 1 child in this age bracket was found to have lead levels between 20-44 BLL
- Only 14.9% of the children were tested
New Jersey law (N.J.S.A. § 24:14A-6) requires Local Boards of Health to investigate all reported cases of childhood lead poisoning (N.J.A.C. § 8:51) within their jurisdiction and to order the abatement of all lead hazards identified in the course of the investigation. The procedures for conducting environmental investigations in response to a lead-poisoned child are specified in N.J.A.C. § 8:51.
The Local Board of Health must conduct an inspection of the child’s primary residence and any secondary address, such as a child care center, the home of a relative or babysitter, or wherever the child spends at least 10 hours per week. If the child moves, the property where the child resided when the blood lead test was performed must be inspected. The environmental inspection includes a determination of the presence of lead-based paint and leaded dust; the identification of locations where that paint is in a hazardous condition such as peeling, chipping, or flaking; and, as appropriate, the presence of lead on the dwelling’s exterior or soil. The inspector, with the public health nurse, speaks to the child’s parent/guardian and completes a questionnaire to help determine any other potential sources of exposure to lead. In addition, the Local Board of Health arranges for a home visit by a public health nurse to educate the parent/guardian about lead poisoning and the steps that he or she can take to protect the child from further exposure. The public health nurse also provides ongoing case management services to assist the family, including but not limited to, receiving follow-up testing, medical treatment, and social services that may be necessary to address the effects of the child’s exposure to lead.